
Requestable on eOrder – No prior approval needed
Effective date: 16/02/2026
What is Fibrosis-4 (FIB-4)?
The FIB-4 (Fibrosis-4) index is a non-invasive score used to stratify liver fibrosis risk in patients with suspected metabolic dysfunction-associated steatotic liver disease (MASLD), previously called non-alcoholic fatty liver disease (NAFLD). It enhances early identification of patients at risk for advanced liver fibrosis using easily accessible, serum-based markers. FIB-4 is recommended by international guidelines due to its simplicity, cost-effectiveness, and particularly its strong negative predictive value for advanced fibrosis. It therefore helps reduce unnecessary imaging or liver biopsy in low-risk individuals.
When should you not request FIB-4?
The FIB-4 score is not recommended for the diagnosis of liver fibrosis in patients with chronic hepatitis C. While it is a useful non-invasive tool for assessing liver fibrosis stages in MASLD (NAFLD), it is not as reliable as liver biopsy (which remains the gold standard for diagnosing liver fibrosis and assessing the severity of liver disease in patients with hepatitis C).
Calculating and interpreting FIB-4
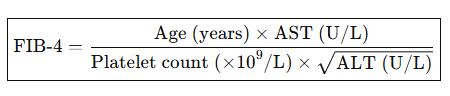
The FIB-4 score incorporates age, AST, ALT, and platelet count and is automatically calculated and reported with associated age-specific interpretive comments and follow-up recommendations. FIB_4 does not have a unit.
- ≤35 years: The FIB-4 score is unreliable in patients <=35 yrs, please interpret with caution. Consider alternative fibrosis assessment.
- >35–<60 years:
- <1.3: Low probability of significant liver fibrosis. Suggest repeat FIB-4 testing in 2-3 years unless clinical circumstances change.
- >=1.3: The FIB-4 score does not exclude significant liver fibrosis.**
- • ≥60 years:
- o <2.0: Low probability of significant liver fibrosis. Suggest repeat FIB-4 testing in 2-3 years unless clinical circumstances change
- >=2.0: The FIB-4 score does not exclude significant liver fibrosis.**
**Where applicable, consider secondary assessment with transient elastography (FibroScan®) and/or hepatology referral to determine the degree of fibrosis, or for further preoperative assessment. https://www.hepatitisfoundation.org.nz/fibroscans/
- There is no universally accepted “critical” FIB-4 value in the same sense as a lab critical value that mandates urgent clinical contact.
- However, thresholds have clinical importance, especially in triaging patients for specialist referral or further imaging (e.g., FibroScan®).
While not a “critical” lab value per se, the following FIB-4 results should prompt specialist referral for review:
- FIB-4 > 3.25: Strongly associated with advanced fibrosis (F3–F4). Many pathways (e.g. NICE, AASLD) use this threshold to escalate care.
- Accompanied by red flags: e.g., elevated bilirubin, low albumin, coagulopathy, clinical stigmata of chronic liver disease—these warrant urgent hepatology input.
References:
- Consensus statement on MAFLD assessment. (2024). Non-invasive testing and FIB-4 utility. https://www.gesa.org.au/public/13/files/Education%20%26%20Resources/ Clinical%20Practice%20Resources/MAFLD/MAFLD%20consensus% 20statement%202024.pdf
- BPAC NZ. (2022). A spotlight on the key causes of chronic liver disease. NZ: Best Practice Advocacy Centre. https://bpac.org.nz/2022/docs/cld.pdf
- Wattacheril, J. J. (2023). AGA Clinical Practice Update: Role of non-invasive tests for liver fibrosis. Gastroenterology. https://www.gastrojournal.org/action/showPdf?pii=S0016-5085%2823%2900881-8
- European Association for the Study of the Liver. (2021). EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis. Journal of Hepatology. https://easl.eu/wp-content/uploads/2021/06/EASL-Clinical-Practice-Guidelines-on-non-invasive-tests-for-evaluation-of-liver-disease-severity-and-prognosis-%E2%80%93-2021-update.pdf
Dr. Melissa Yssel
Clinical Lead – Chemical Pathology & Illumiscreen
Awanui Labs