
Updated Courier Sample Collection
We are updating courier sample collection procedures across all medical centres to align with industry practices and improve patient privacy and scheduling.
From Wednesday, 1 April 2026:
- All collections will occur at one designated pickup point at the front reception desk
- Couriers will no longer enter clinical or non-public areas
- Samples must be ready at reception before scheduled pickup
Medical practices are responsible for storing and managing samples until collection. If you need a suitable container, please email WLG.Admin@awanuilabs.co.nz.
Thank you for your support.
Easter and April School Holiday opening hours
The opening hours for our collection centres during the Easter and the April school holidays (3-18 April) can be found on our website here.
Guidance on Allergy Testing: Choosing Wisely for Better Outcomes
Awanui Labs is updating its approach and guidance for referrers on allergy testing to promote clinically appropriate use, reduce harm from over testing, and support equitable access. The focus is on using tests only where results will change management, avoid unnecessary restriction of well tolerated foods, and methods to fit a modern, automated laboratory environment.
New Zealand has one of the highest burdens for allergic disease in the world with over 40 percent of the population being classified as atopic, which is defined as having positive specific IgE, or skin prick testing to common environmental allergens. Given how common atopic disease is in this country, it is important clinicians maintain a good working knowledge of the assessment of asthma, eczema and allergic rhinitis and where allergy testing is helpful in the diagnosis and management of these conditions.
In this guide, Awanui Labs Chief Medical Director Richard Steele discusses different principles for ordering allergy tests within the Awanui laboratory network to support the optimal use of allergy testing saving time, cost, and delivering the right outcomes for your patients.
These key principles are outlined below to guide safe, and effective practice.
Principle 1: Test Only in the Right Context
Allergy testing is a finite resource and should be reserved for situations where there is a clear clinical indication and the result will guide management.
Figure 1 (Indications for Allergy Testing) outlines when IgE mediated allergy testing is appropriate and emphasises that testing outside these indications can lead to harm.
Indications for allergy testing, asking the right questions
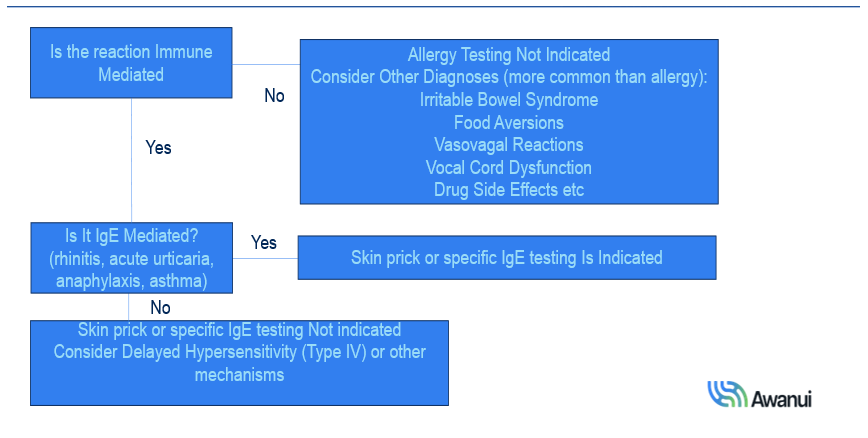
- Aeroallergens: Testing should be limited to patients with persistent, recurrent, severe rhinitis or asthma not controlled on standard therapy and only where results will influence treatment decisions. It is not indicated for eczema in primary care and is only rarely helpful in specialist practice unless there is significant allergic rhinitis or asthma present.
- Food allergens: Testing is appropriate when there is a history suggestive of an IgE mediated immediate reaction and the patient is currently avoiding the food. Skin prick and specific IgE are both valid modalities, however, oral food challenge remains the gold standard when the diagnosis is uncertain.
- Indiscriminate food testing: Broad, non-targeted food panels frequently detect sensitisation in patients who are clinically tolerant, driving unnecessary food avoidance and nutritional risk, especially in children. One study of 274 patients undergoing indiscriminate serum food panels generated about US$80,000 in excess health care costs, with many individuals sensitised on testing but ultimately not diagnosed with food allergy after specialist evaluation.
- Maintaining regular oral exposure to tolerated foods is critical, as stopping these foods on the basis of a positive test alone can increase the risk of developing true IgE mediated food allergy, including anaphylaxis. Testing is not indicated for non IgE mediated conditions such as irritable bowel syndrome, and for eosinophilic oesophagitis or oral allergy syndrome, broad food testing is unhelpful. In oral allergy syndrome, birch pollen testing alone is recommended to support the diagnosis.
Principle 2: Specific IgE or skin prick testing can be used but not both
For IgE mediated allergy, clinicians should choose either serum specific IgE or skin prick testing for a given allergen but not order both, as using both does not improve diagnostic accuracy and adds unnecessary cost and complexity.
Both modalities have broadly similar diagnostic performance and should be selected according to patient factors and system constraints. Specific IgE is often preferable when there are equity barriers to attending skin prick testing appointments, when patients cannot stop antihistamines, in dermographism, or when the relevant allergen (for example certain tree nuts or molluscs) is not available as a skin prick. Skin prick testing, while offered through Awanui, is inherently manual, more prone to technical and transcription errors, and carries a small risk of systemic reactions or vasovagal events requiring immediate attention.
Specific IgE testing is well suited to the modern laboratory: it is fully automated, electronically ordered and resulted, and removes many of the manual steps that introduce error. From clinical, operational and financial perspectives, Awanui is therefore shifting toward specific IgE as the preferred modality where this makes sense, with the balance between methods to be reviewed over the next six months
Principle 3: Allergy test ordering in primary care should be limited to the common clinically relevant allergens encountered
In primary care, both the range and number of allergens tested should be limited, and Awanui will implement this policy in 2026. Professional bodies such as the American Academy of Allergy, Asthma and Immunology recommend restricting broad allergen panels to allergy specialists or general practitioners with appropriate extra training.
- Recommended aeroallergens for primary care: House dust mite, grass mix, cat, dog, birch, plantain and a mould mix, with a maximum of 7 aeroallergens per patient.
- Recommended food allergens for primary care: Peanut, wheat, milk, egg, soy, selected tree nuts (almond, Brazil nut, cashew, hazelnut, macadamia, pecan, pistachio, walnut) and common seafoods (e.g. codfish, shrimp, mussel, lobster, oyster, tuna, salmon, crab, scallop), with a maximum of 3 food allergens per patient
Access to a broader range of tests should be limited to clinicians with demonstrated allergy expertise (such as clinical immunologists, immunopathologists, allergists, paediatricians, or GPs with extended allergy roles), use within agreed Health Pathways, or GPs who have completed approved allergy training modules. This approach is designed to reduce over diagnosis, minimise harm and unnecessary resource use, and direct complex cases to appropriately trained clinicians.
For further information, please see details below, the Awanui Test Guide or discuss with an Awanui Labs Immunopathologist.
- For Aeroallergens, allergy testing should be reserved only for those with persistent, recurrent and severe rhinitis or asthma symptoms not controlled with standard therapy AND the results will guide management.
- Specific IgE or skin prick testing can be used to test for the same allergen but do not order both.
- Allergy test ordering in primary care should be limited to the common clinically relevant allergens encountered.
- Positive tests without allergy (sensitisation) occurs 5 times more commonly than true allergy.
- The positive and negative predictive value for a given wheal size or specific IgE antibody level will vary for each individual allergen and for most allergens that is not known.
- The positive and negative predictive value for a given wheal size or specific IgE antibody level will vary for each individual allergen and for most allergens that is not known.
- Larger wheal size or higher the specific IgE level the more likely a person is allergic to that particular allergen BUT does not predict the reaction severity.
- There is no definite cut off for either wheal size (<3mm) or specific IgE level (<0.35kUA/l) they are arbitrary.
- True allergy can occur at levels lower than the cut-off.
- Skin prick testing in children, a small wheal (sometimes <3mm) with a very large flares\ is commonly seen in true allergy.
- For foods, a specific IgE level less than 0.1kAU/l or a negative skin prick test has a high negative predictive value that the patient is not allergic BUT it is only a test and specialist advice should always be sought when re-introducing the food in question where there is a history of a previous IgE mediated reaction.
- For foods, allergy testing should only be performed in those with a history of an acute IgE mediated reaction who is currently avoiding the food in question.
- If a patient has a positive allergy test to a food they are currently tolerating, they should be encouraged to continue to eat that food on a regular basis. Cessation may lead to true IgE-mediated allergy including anaphylaxis.
- Multiple negative results (usually house dust mite, cat, dog, birch, grasses, plantain) with no positive results it is very unlikely that atopy is a factor contributing your patient’s symptoms e.g. allergic versus non-allergic rhinitis or in asthma.
- For pollens, all the relevant allergens (e.g. grasses, plantain, birch) are introduced species that produce airborne pollens.
- No native plant (pollinated by insect or bird spread) has ever been demonstrated to cause allergy.
View the email version here.