
Antibiotic susceptibility patterns (antibiograms)
The data provided below is for all Awanui Labs sites.
Antibiotic susceptibility patterns (longitudinal data) 2025
Escherichia coli
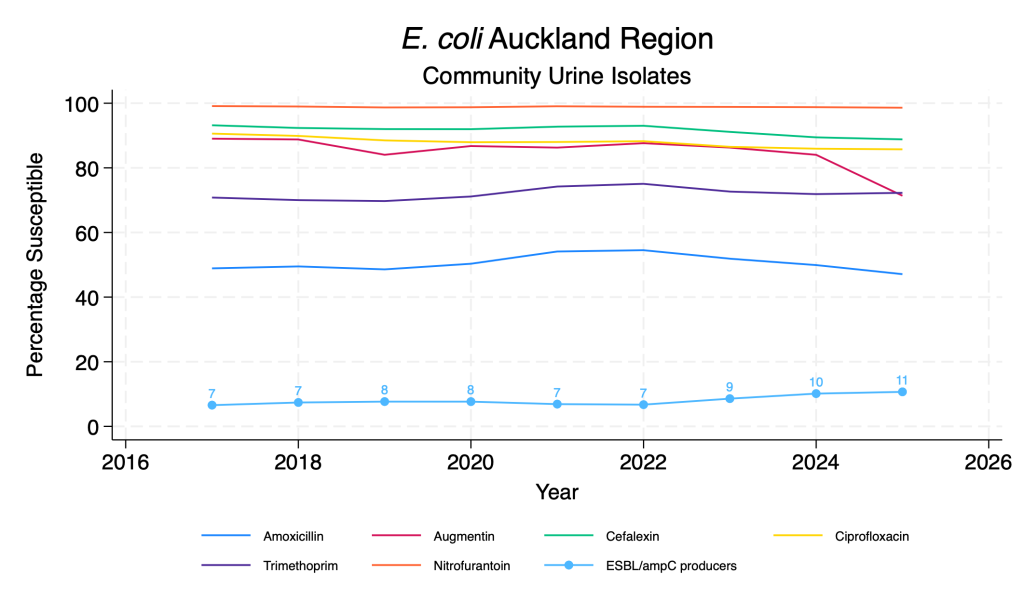
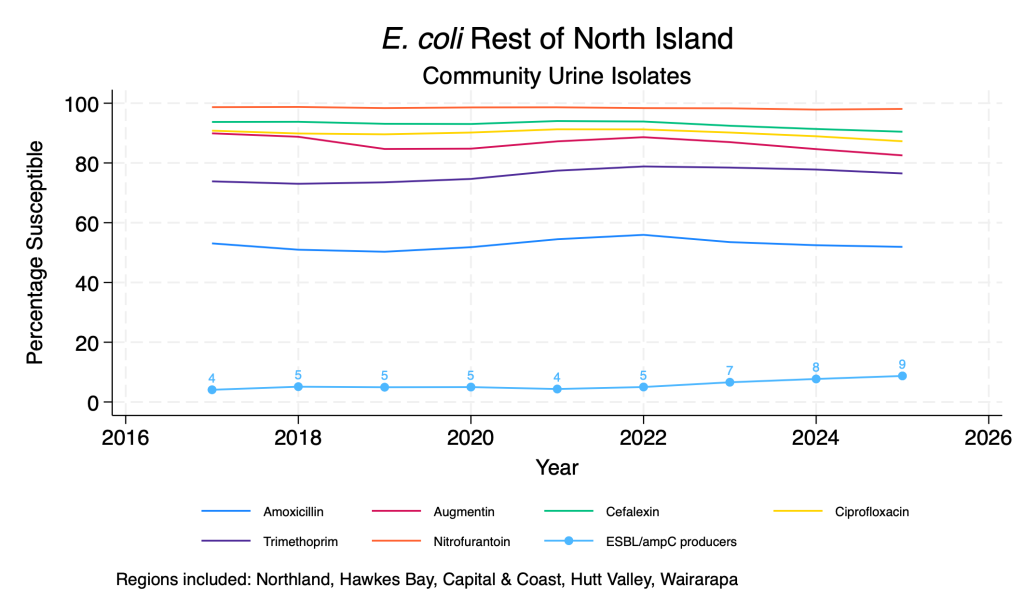
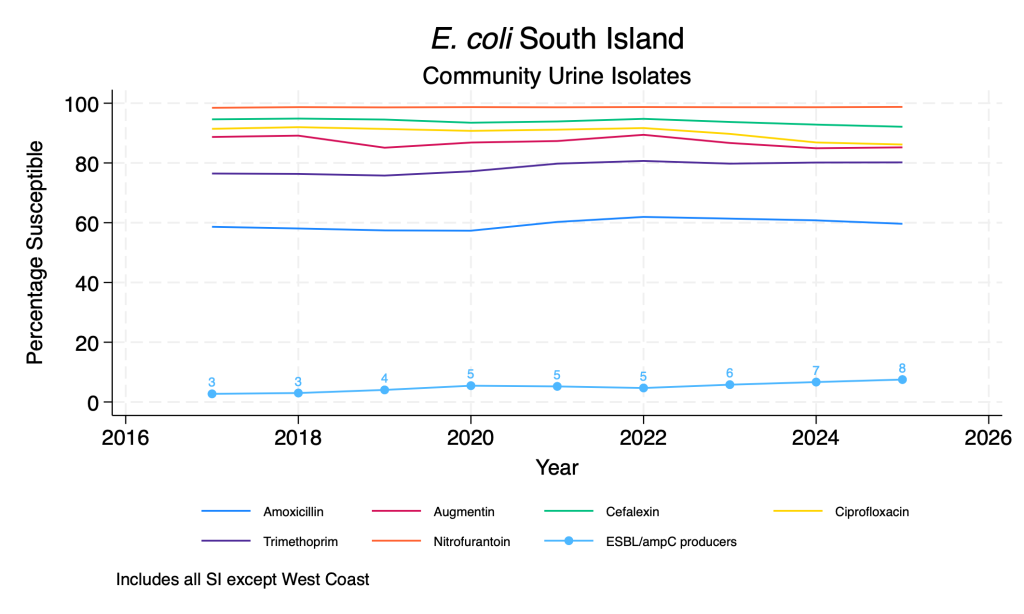
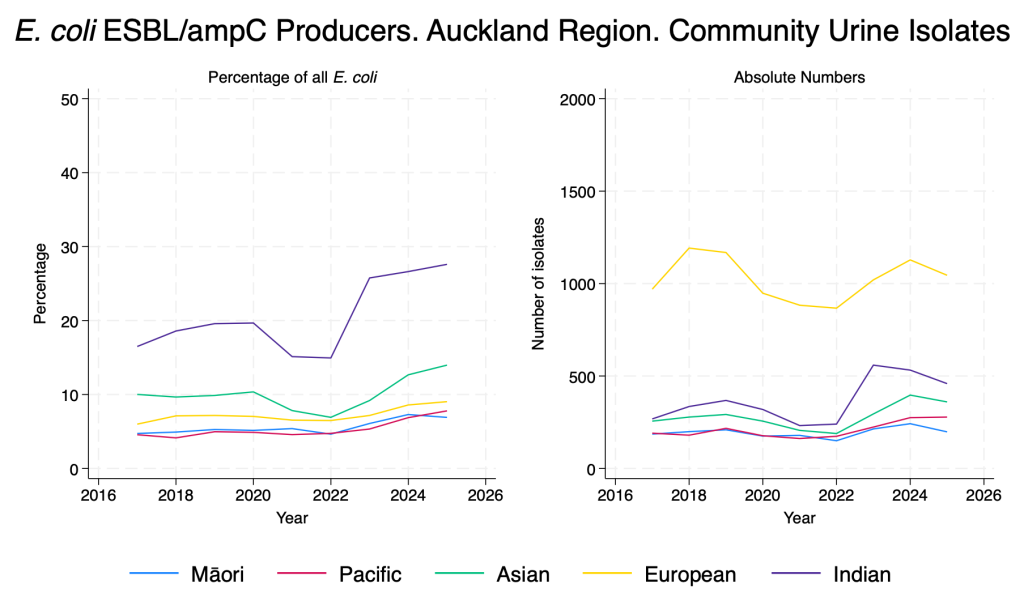
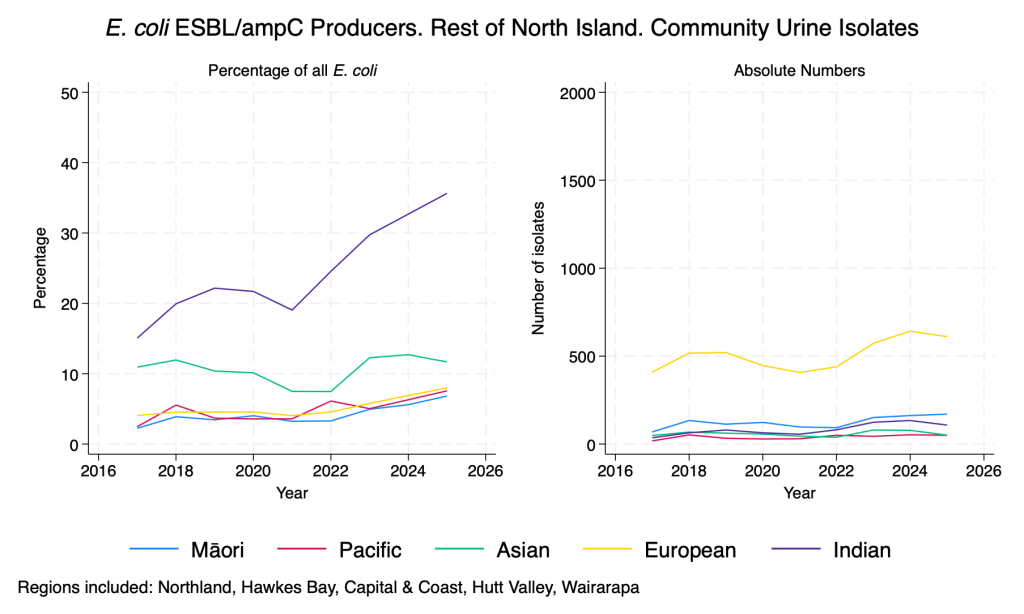
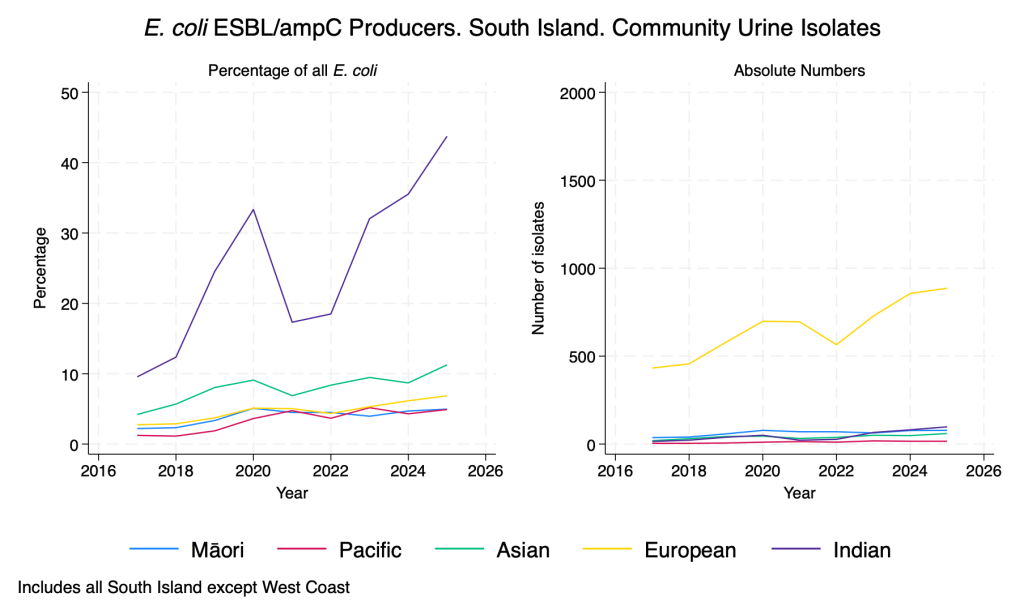
Data derived from community urine samples. E. coli is the commonest urinary isolate by a huge margin. Duplicate isolates from the same person in the same year with the same resistance pattern are removed. ESBL/ampC production is inferred from resistance to any third-generation cephalosporin. Percentage of isolates with ESBL/ampC production is also presented by prioritised ethnicity, due to the known association between gram negative resistance and ethnicity in the NZ context.
Commentary
- Susceptibility to the common E. coli oral agents is relatively stable over time across the regions although there are some regional differences.
- Nitrofurantoin resistance remains very rare, despite significant increases in usage over time.
- There does appear to be an ongoing slow rise in the proportion of isolates that are ESBL or ampC producers across the regions.
- When examined by ethnicity there are pronounced differences in the proportion of isolates with ESBL/ampC production, particularly in those of Indian ethnicity, in whom the proportion is rising rapidly.
E. coli main agents – community urine isolates
E. coli ESBL/ampC producers – community urine isolates – by ethnicity
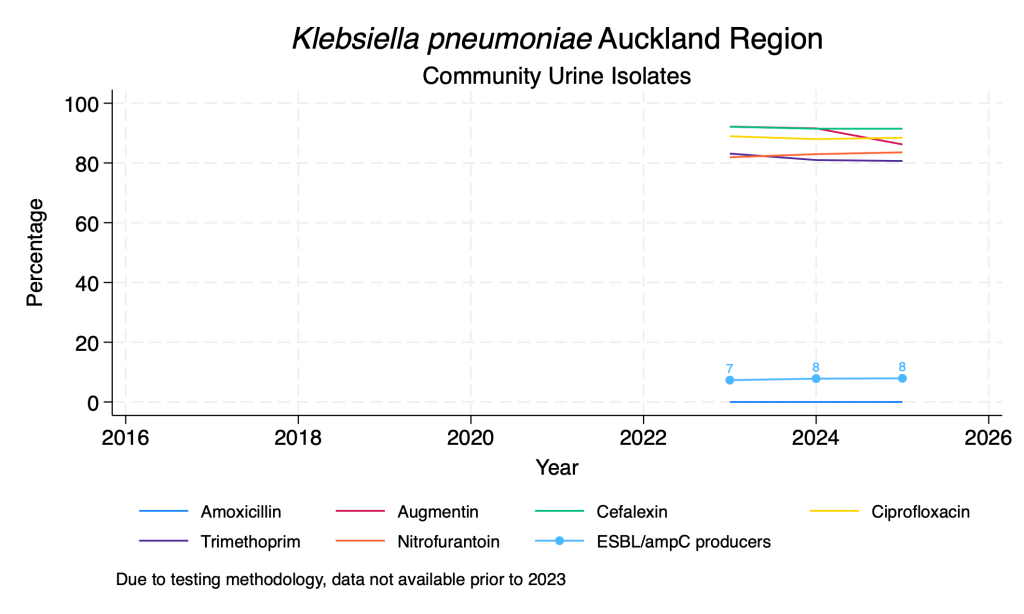
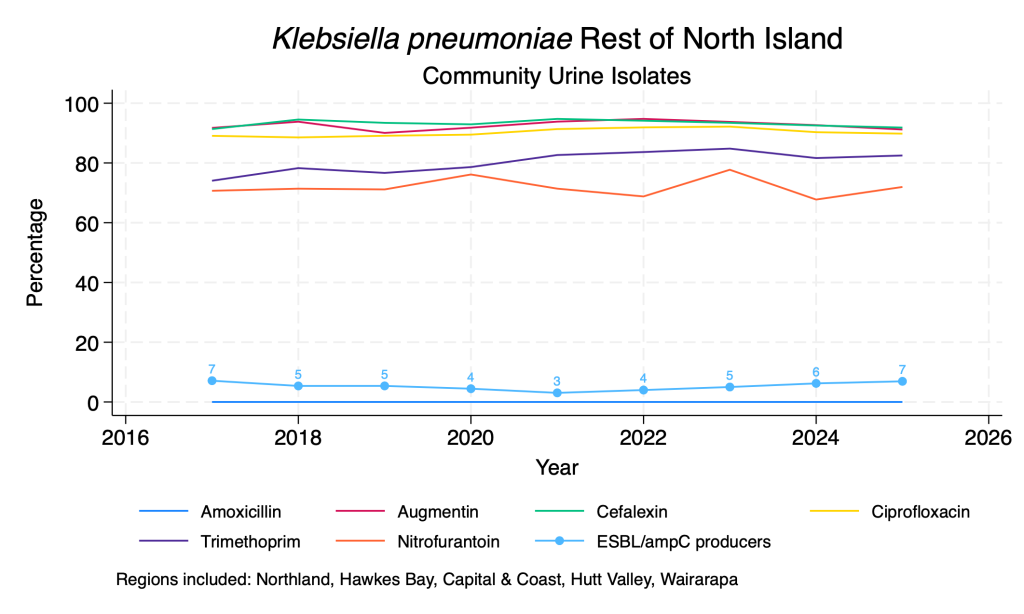
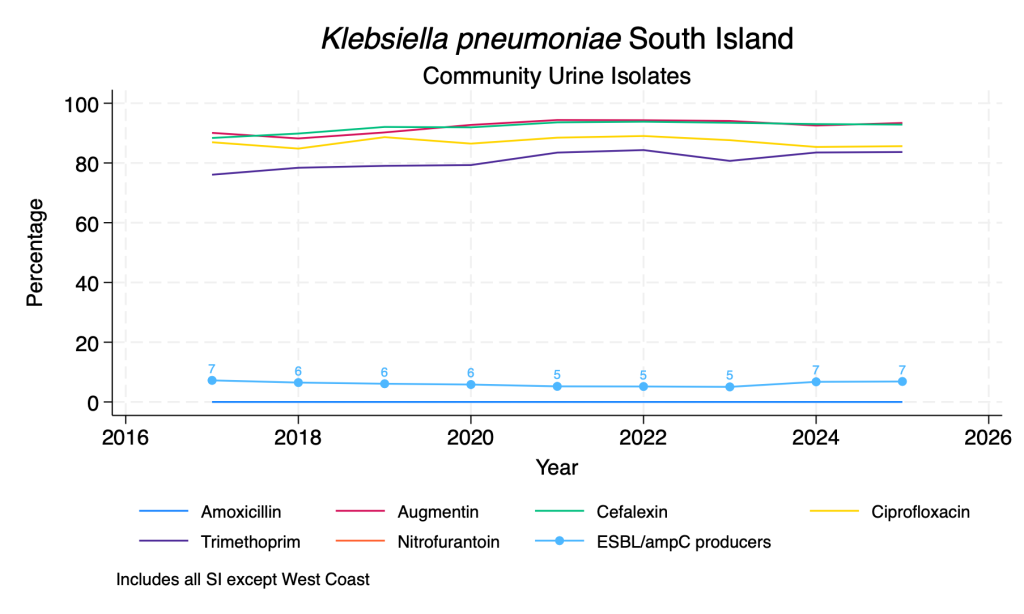
Klebsiella pneumoniae – community urine isolates
Data derived from community urine samples. K. pneumoniae is the second commonest urinary isolate. Duplicate isolates from the same person in the same year with the same resistance pattern are removed. ESBL/ampC production is inferred from resistance to any third-generation cephalosporin. Due to lower numbers, ESBL/ampC production by ethnicity is not reported.
Commentary
- Susceptibility to the common oral agents is relatively stable over time.
- The proportion of isolates with ESBL/ampC production has seen minor fluctuations over the time period, with the suggestion of a slow rise over the past 3-4 years.
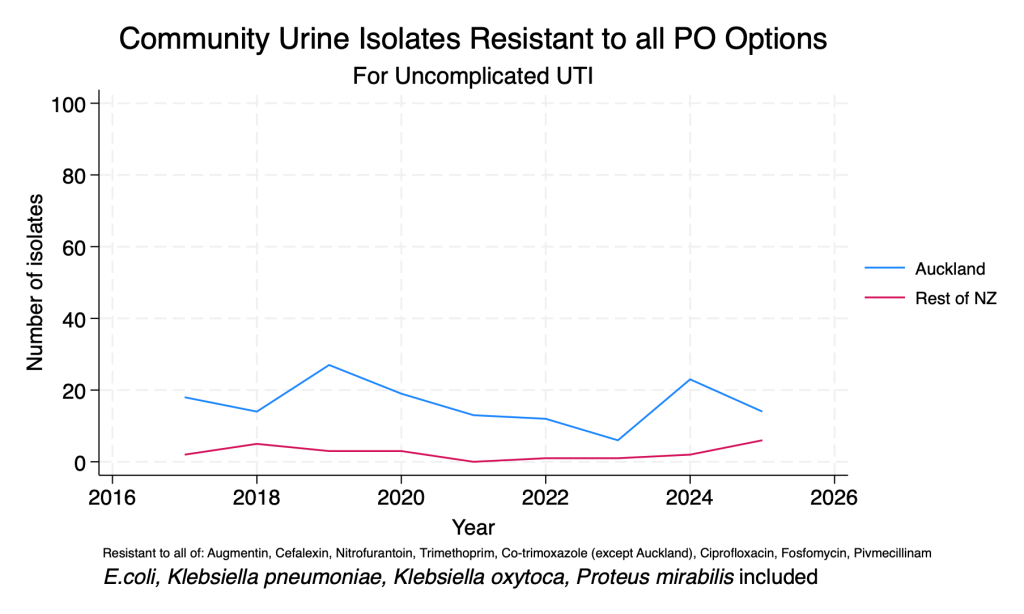
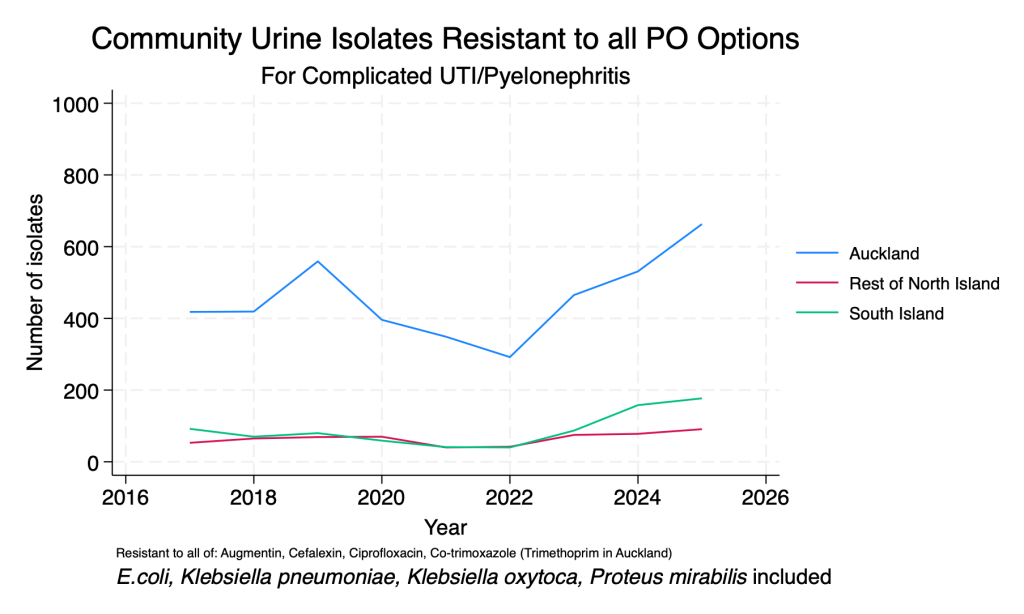
Difficult to treat urine organisms
These data are presented to demonstrate the effects of AMR on the ability to treat common UTI organisms in the community setting. Difficult to treat organisms increase the risk of empiric treatment failure and may mean UTIs that could otherwise be treated with oral therapy require intravenous therapy. To be included, organisms must have been tested for all of the listed agents, which means numbers may fluctuate over time due to changes in lab methods.
Commentary
- Organisms testing resistant to all available oral agents suitable for uncomplicated UTI (i.e. cystitis) remain very rare in the community setting. A significant contributor to this is the reliability of nitrofurantoin.
- Organisms testing as resistant to all available oral agents suitable for treating complicated UTI are more common, with recent increases in absolute numbers. These results are derived from all urinary isolates (it is currently difficult to determine based on laboratory data on a large scale which patients have complicated UTI), so they are indicative only.
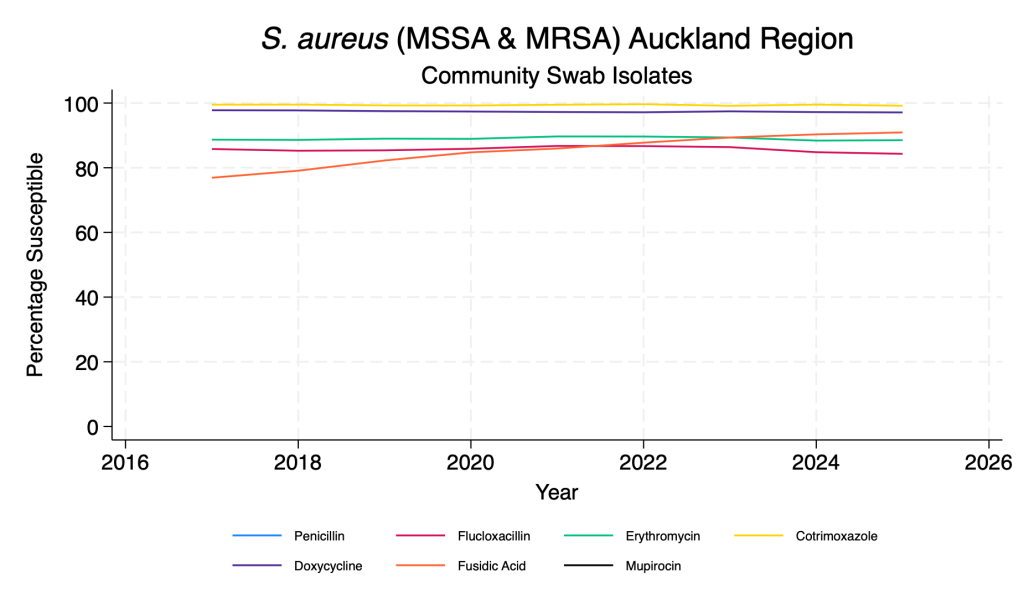
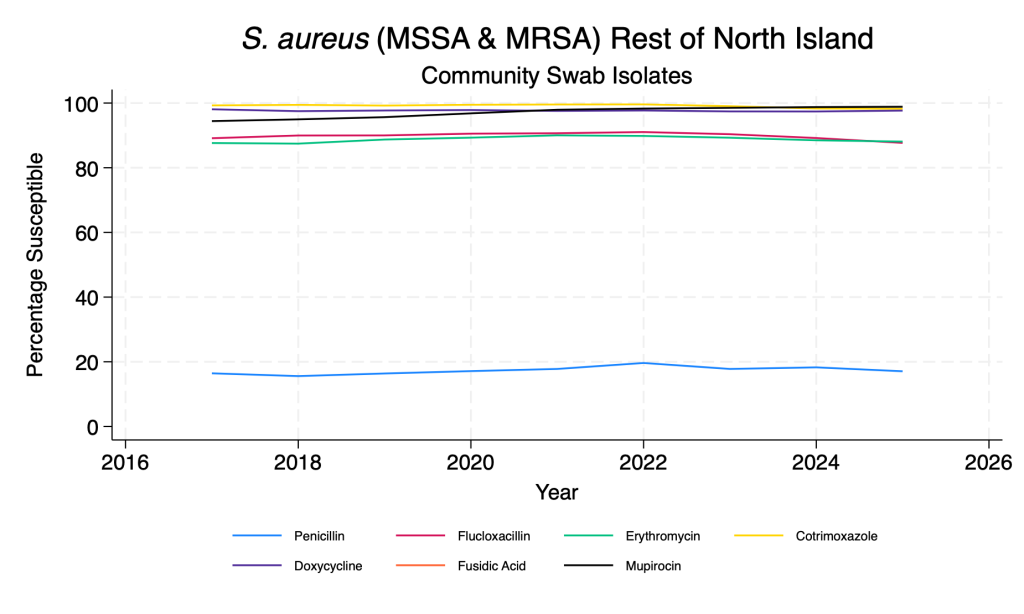
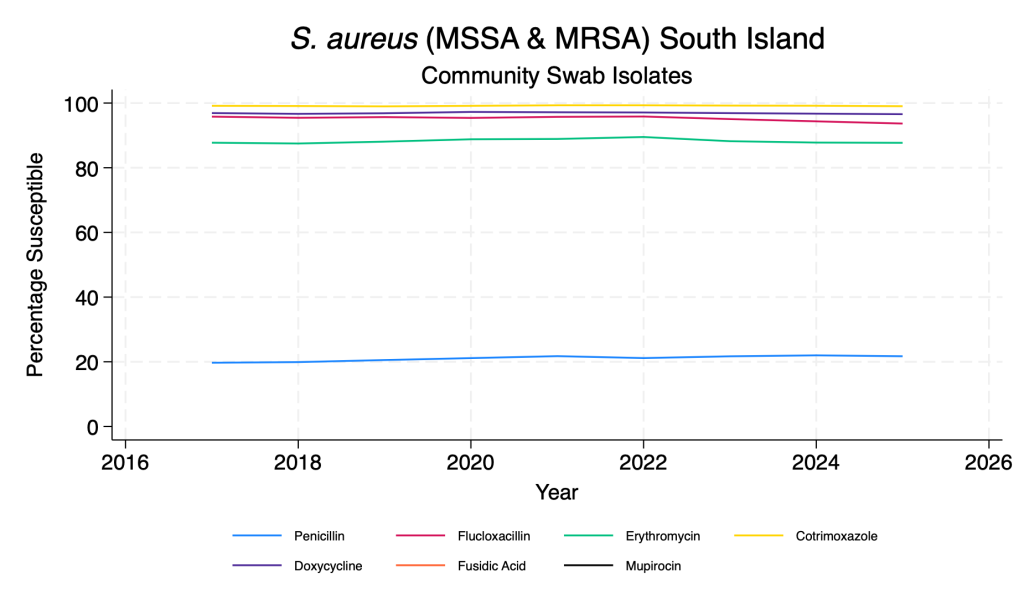
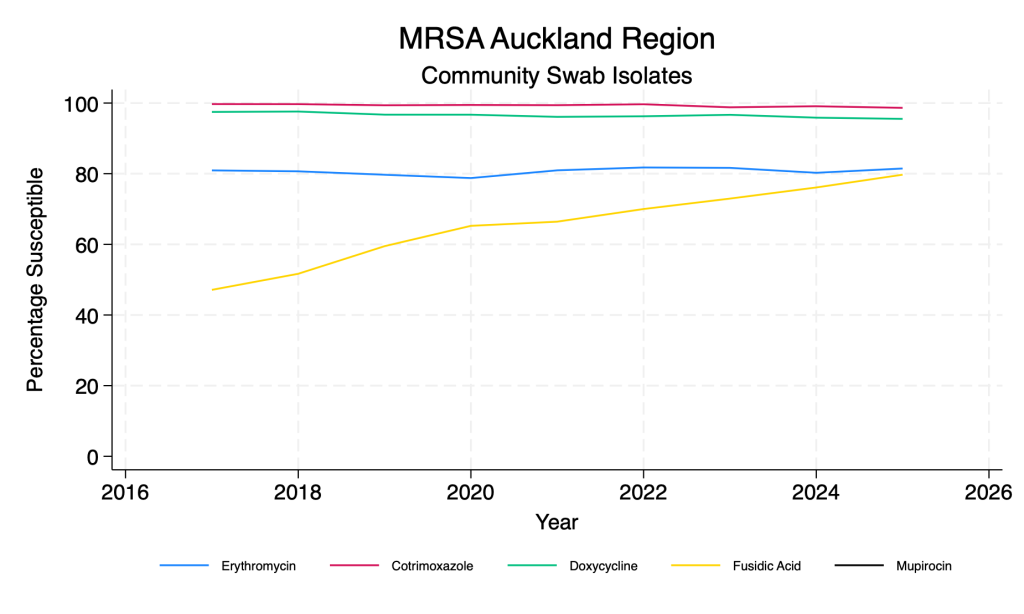
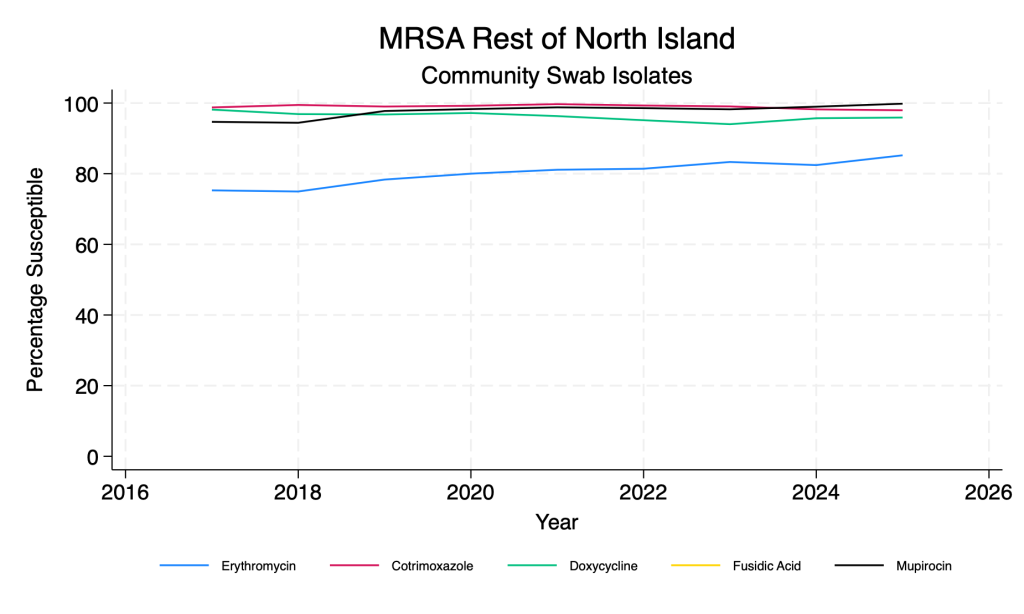
Staphylococcus aureus
These data are derived from community swab samples. S. aureus is by far the commonest Gram-positive organism isolated. Duplicate isolates from the same person in the same year with the same resistance pattern are removed. Data are presented here for all S. aureus (methicillin susceptible and resistant – MSSA and MRSA) and for MRSA only.
Commentary
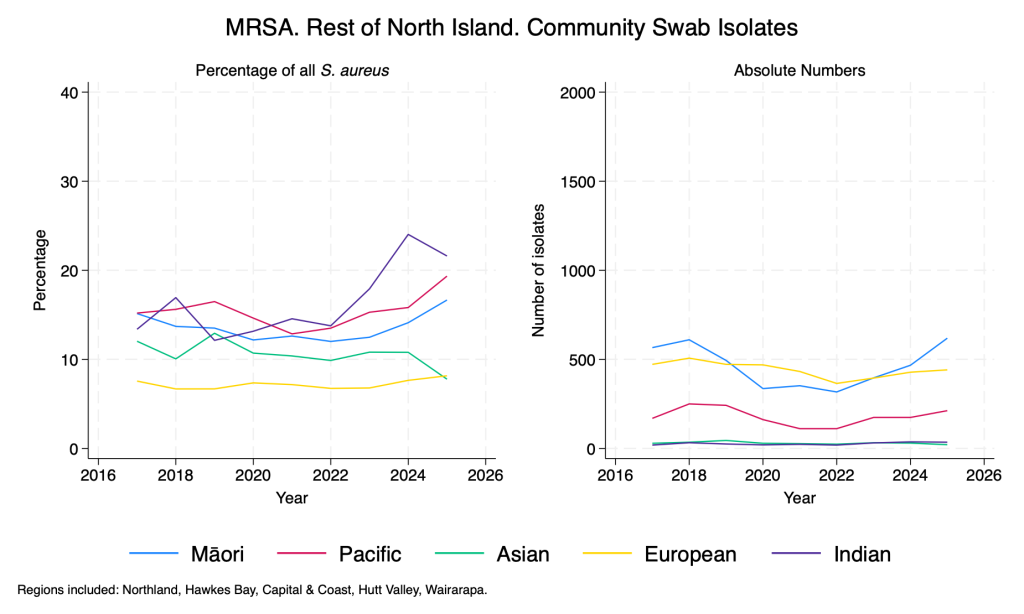
- In the past 2-3 years there has been a gradual reduction in flucloxacillin susceptibility (i.e. an increase in MRSA). MRSA is more common further north in New Zealand.
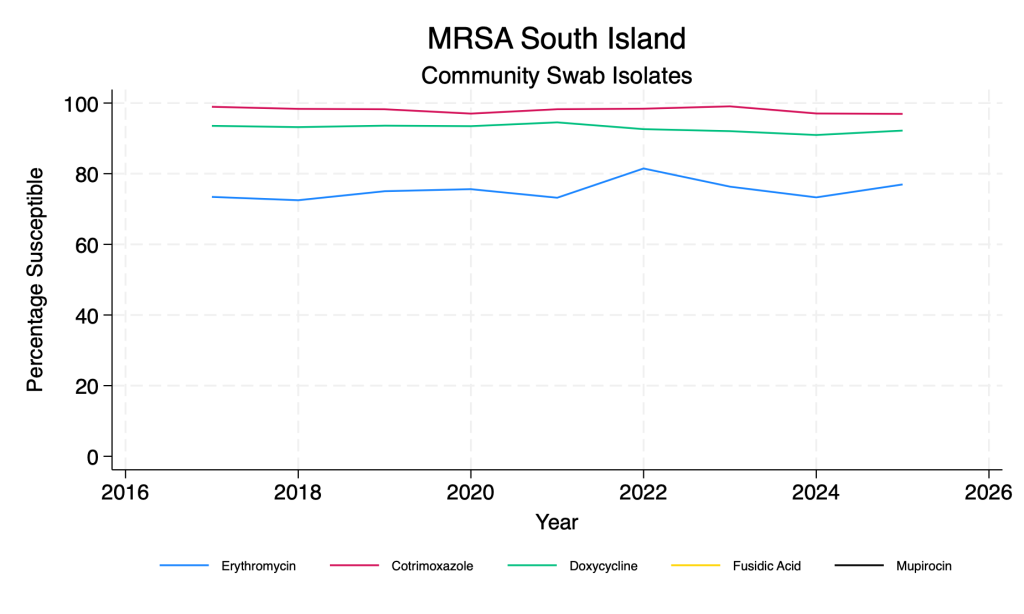
- Fusidic acid susceptibility has improved dramatically across the time period.
- Co-trimoxazole and doxycycline remain reliable agents for both MSSA and MRSA.
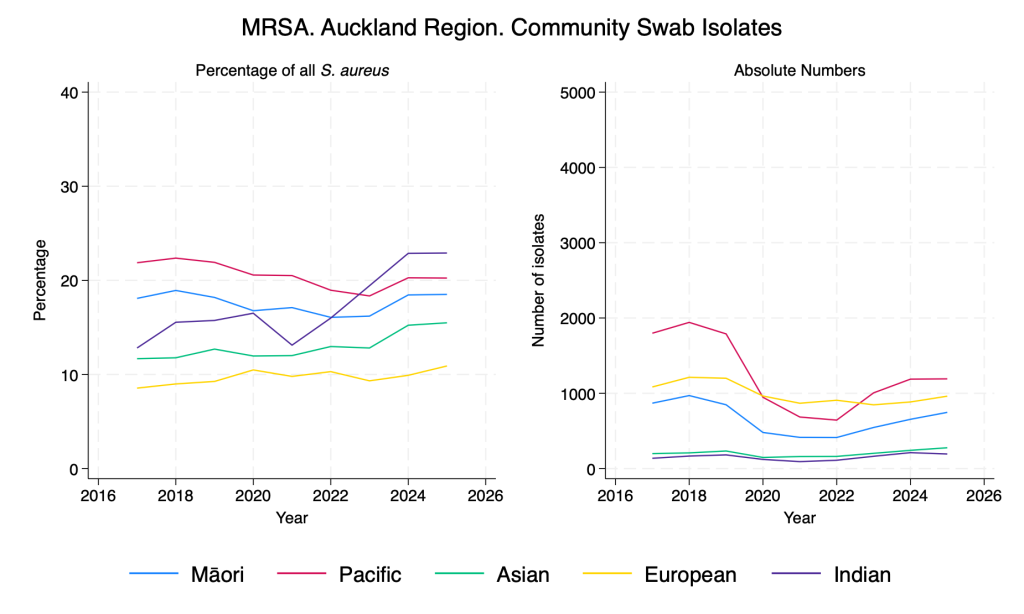
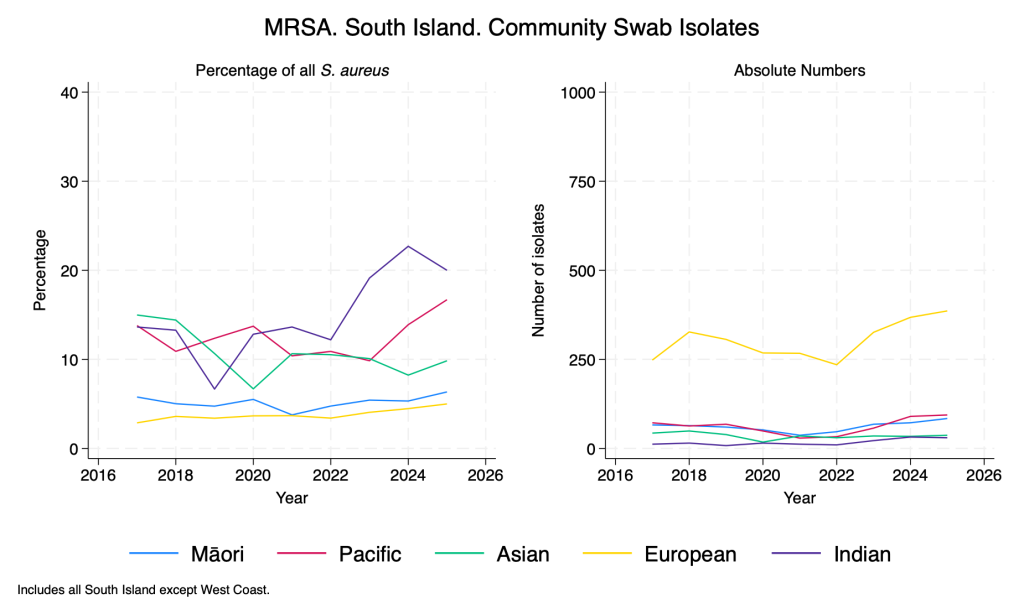
Similar to Gram-negative resistance, there are clear differences in the proportion of S. aureus isolates that are MRSA according to ethnicity, with recent significant rises in those of Indian ethnicity.
Staphylococcus aureus – main agents – community swab isolates
MRSA – main agents – community swab isolates
MRSA – community swab isolates – by ethnicity
Bloodstream infection isolates
Coming soon.
Antibiotic therapy
Recommended adult doses for ‘optimised’ antibiotic dosing
Note: many of these agents may require adjustment with significant renal impairment. Seek ID or pharmacy advice if necessary.
Oral agents:
- Amoxicillin – 1g tds
- Augmentin – use ‘boosted augmentin’ (Augmentin 625mg tds + amoxicillin 500mg tds)
- Ciprofloxacin – 750mg bd
- Co-trimoxazole – 1440mg bd or 960mg tds
IV agents:
- Amoxicillin – 1g q6h (standard dose sufficient for ‘I’ when given IV). If patient septic or >100kg use 2g q6h.
- Augmentin – 1.2g q8h (standard dose sufficient for ‘I’ when given IV). If patient septic or >100kg use ‘boosted IV augmentin’ (Augmentin 1.2g q8h + Amoxicillin 1g q8h)
- Benzylpenicillin 2.4g q6h
- Ceftazidime – 2g q8h
- Cefepime – 2g q8h
- Piperacillin-tazobactam (Tazocin) – 4.5g q6h
Topical treatment options for conjunctivitis
| Chloramphenicol | Fusidic Acid | Tobramycin | Ciprofloxacin | |
| Staph aureus | Susceptible | Susceptible | Susceptible | Susceptible |
| Haemophilus influenzae | Susceptible | Resistant | +/- | Susceptible |
| Strep pneumoniae | Susceptible | Resistant | Resistant | +/- |
| Moraxella catarrhalis | Susceptible | Resistant | Resistant | Susceptible |
| Corynebacterium macginleyi | Susceptible | Resistant | Resistant | Susceptible |
| Pseudomonas aeruginosa | Resistant | Resistant | Susceptible | Susceptible |
| Enterobacterales (e.g. E. coli, Klebsiella, Serratia) | Susceptible | Resistant | Susceptible | Susceptible |